
What kind of moron schedules an appointment with a new specialist while recovering from yet another revision to breast reconstruction? Probably the same moron who thinks yet another revision is no big whoop and expects recovery to be swift. Will I never learn??? And the post-surgery antibiotics are wreaking their usual havoc and using black magic to cause me — a non-meat-eater and pet-pig owner — to crave ham. Ham. Of all things.
Dr E, the neurologist I saw yesterday for the mystery neuropathy I’ve been having in my hands, offices in the medical plaza adjoining the hospital to which I was admitted in early June 2010 for the nefarious post-mastectomy infection. A small PTSD episode may or may not have occurred inside that plaza at 8:30 a.m. yesterday, in which I stepped on to the wrong elevator en route to Dr E’s office and found myself not in the plaza but on the 9th floor of the hospital. I was transfixed and rooted in place, knowing I was not in the right spot but temporarily unable to grind the right gears and get out of there. I stood there, sweating profusely and shivering alarmingly near a giant window overlooking the freeway that leads from the hospital back to my home, in the Land of Sugar. The dregs of a rainy-day morning rush hour in Houston creeped along that freeway as I watched it, momentarily paralyzed with the searing memory of looking out that window on day 6 or 7 of that hellish hospitalization. My kids had just finished their second- and fifth-grade years of school; I had turned 41 just a week before that hellish hospitalization. Summer glistened ahead of us as I began a protracted and ugly battle against a rare and nasty infection following a cruel and unexpected cancer diagnosis. If someone had predicted that nearly 5 years later I would be paralyzed simply by being in that same hospital, I would have rolled my eyes and scoffed at that lame-0 idea. Suffice to say, no eye-rolling or scoffing occurred.
 I sweated and cursed the small, airless room. I wondered how much time had elapsed. I wondered if clicking that button was contributing to the neuropathy in my hands. I rebelled against the test directions to avoid looking for a pattern and guessing when to click the button. I composed a grocery list. I fashioned a crude fan from a piece of paper to stir the hot, stale air, not once taking my eyes off that blasted screen. I thought about what to serve my kids for dinner that constituted a nutritious meal yet required little or no work from me. I vowed to ace that test, but grew bored of and distracted from it post haste. Hence the no filter.
I sweated and cursed the small, airless room. I wondered how much time had elapsed. I wondered if clicking that button was contributing to the neuropathy in my hands. I rebelled against the test directions to avoid looking for a pattern and guessing when to click the button. I composed a grocery list. I fashioned a crude fan from a piece of paper to stir the hot, stale air, not once taking my eyes off that blasted screen. I thought about what to serve my kids for dinner that constituted a nutritious meal yet required little or no work from me. I vowed to ace that test, but grew bored of and distracted from it post haste. Hence the no filter.
googleimages.com
But instead, I was like this (pardon the profanity; it’s fitting and again, another example of me having no filter):
googleimages.com
Today is my favorite day of the year. No, it’s not my birthday — it’s Global Champagne Day. Which might as well be my birthday. It’s one good thing — perhaps the only good thing — about the month of October, and I plan to celebrate. 
Some people consider December 31st to be GCD; however, they are wrong. December 31st is New Year’s Eve, and while lots of champagne is consumed on that day every year, champagne does not share the limelight with the last day of the year, with the giant mirrored ball dropping, or any such nonsense. Champagne stands on its own. Sheesh, the fact that it’s Global Champagne Day proves that. It’s not even in the same league as National Shrimp Day or National Lost Sock day.
One of my friends at the gym heard me talking about GCD and asked — in all sincerity — if I made it up. As if I would fabricate a global movement just to have an excuse to drink champagne. As if I need a reason. Sheesh.
In honor of my favorite beverage on my favorite day of the year, here are some of my favorite quotes. I’d love to find bigger images of these quotes (all from googleimages.com) but am in too big of a hurry to pop a cork. Perhaps there is a way to edit the sizes right here on my computer screen, but again…time’s a wasting and I gotta get to pouring.
I gotta work on that “start with a smile part.” The “finish with champagne” part — I got it covered.

I couldn’t agree more with Napoleon. And that guy knew a thing or two about defeat. Drink up, people.

It makes no matter if one is happy, sad, alone, with others, thirsty or sated. Champagne is just right for every occasion. Promise.
I like to drink water along with my champagne, so I can keep drinking the bubbles without fear of waking up with a headache. It’s called The Water Course, and anyone who has raised a glass with me knows I swear by that practice. A little tip from me to you. You’re welcome.  Dance away, folks. Just don’t spill your champagne.
Dance away, folks. Just don’t spill your champagne.
I have this Bette Davis quote framed and hanging in my bathroom, where I see it every day. Most of the times I see it, it makes me thirsty. 
I have no clue who Cat Deeley is, but he or she is wise. Very wise.
Allow me to reiterate: champagne is just right for any occasion.
Preach on, Mark Twain. Preach on.

Oh, Winston Churchill! Why oh why didn’t anyone listen to you and institute a free champagne policy?
I don’t care what the question is, 
Seriously. It does not matter what the question is. I know the answer.  Don’t let this happen to you.
Don’t let this happen to you.
Cheers, y’all!
Lovely surprises lurk around every corner.
Sounds like a corny message from a fortune cookie, right? Certainly not what you expect from this little blog, which is typically full of snark. Allow me, if you will, to deviate from the gnashing of teeth, shaking of fists, and renting of garments usually contained within this site.
I had an appointment at the med center this morning to have my wonky thyroid checked out. I love the fact that I live in a city that is home to the world’s largest medical center and that world-class care is available to me.
Some fun facts about the med center:
Indeed, everything is bigger in Texas.
Ok, so being the most kick-ass med center isn’t enough. TMC also throws up some pretty nice artwork–hence the lovely surprise. This morning while hoofing it from the endocrinologist’s office to the radiology department (a portion of the 1.5 square miles mentioned above) for an ultrasound, I passed some unusual artwork and stepped in for a closer look. Picasso said, “The purpose of art is washing the dust of our daily life off our souls,” and I was all for giving my soul a little spit-shine.
The minimalist approach of the first piece caught my eye, with its interesting color combination and deft brushwork. The combination of long, thin brushstrokes and fat, wide ones hold a lot of appeal. 
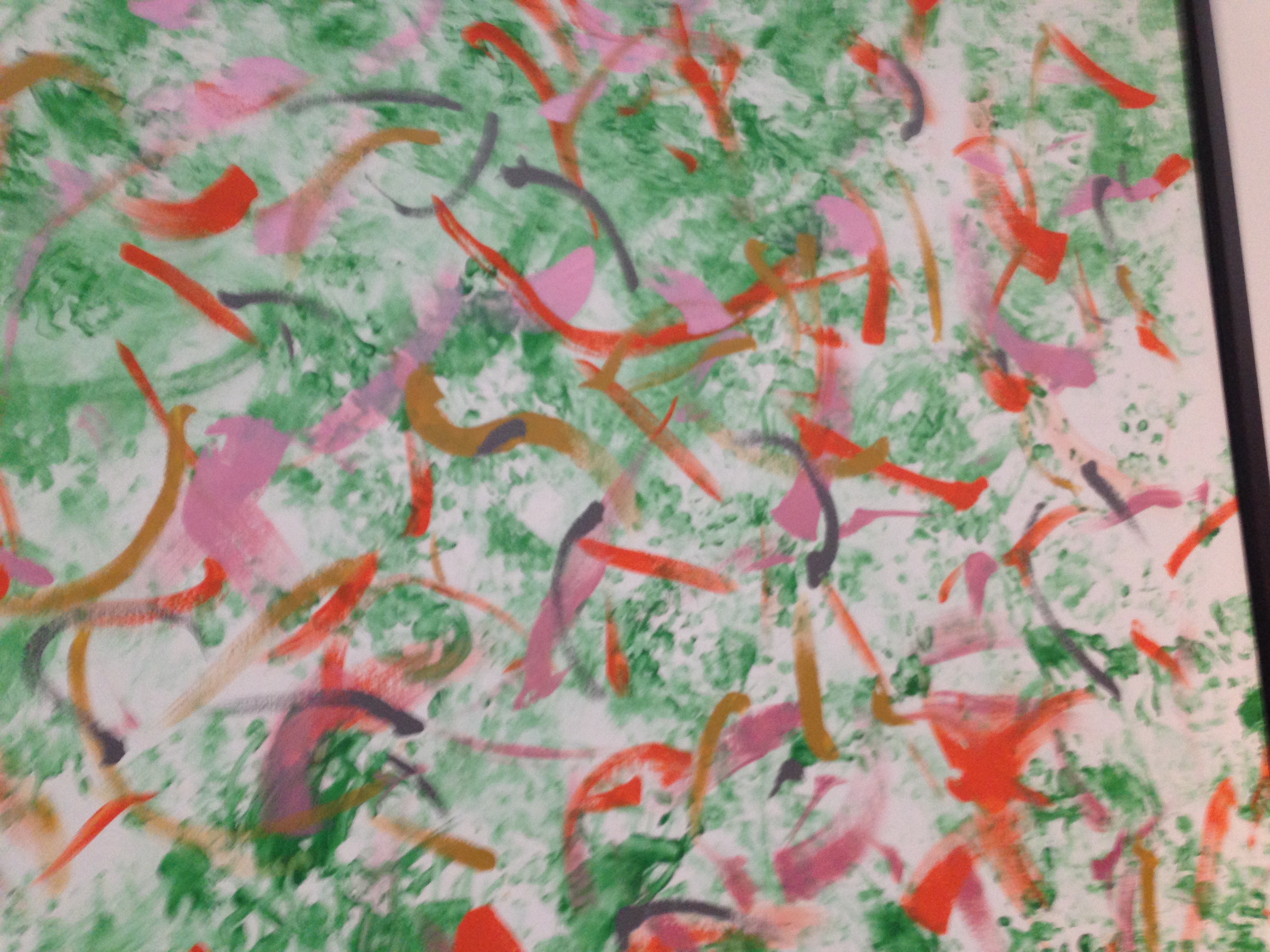
The second piece is much busier and conveys a very different energy. The squiggles suggest movement and a fast pace, and the composition suggests the artist has a lot to say and says it quickly.
Painting number 3 is a bit more purposeful and controlled. The brushstrokes suggest a certain scale to me, and my first instinct is big. Or perhaps the suggestion of large size comes from the predominance of orange, which to me is a color that speaks out loud.

Back to a minimalist style for the fourth piece. The ratio of color to white space is quite different from the other pieces. While the pieces share a similar color scheme, they are vastly different.

The fifth painting could have been done by the same artist as painting number 4, with its similar colors and use of white space. The restraint that comes from the white space impresses me, as my instinct would be to cover a canvas with as much color as possible. Restraint has never come naturally to me. 
Hmmmm. Very intriguing. I’m no art critic, but I like what I see, and I definitely like these pieces.
Would you believe that each piece was painted by a resident of the Houston Zoo?
The first piece was painted by Shanti, an Asian elephant who, according to her artist bio, is pretty serious about her craft. She dips her paintbrush into sand to give her paintings a mixed-media effect, and unlike the other elephant artists, she curls her trunk around the brush rather than holding it with the “finger” at the end of her trunk. She employs a keen concentration while painting and then likes to unwind by horsing around in the pool (she’s known for swimming in circles to make waves while the other members of her herd are in the pool).
The “busy” feel of painting number 2 can likely be attributed to its artist: an otter named Wednesday. This playful painter likes to walk through a puddle of paint and then step onto her canvas, hence the stippled look of the predominant green paint. She has been known to take a break from painting to go for a swim, then return to her canvas and let her wet feet create a true watercolor. Her motto: Will paint for fish.
The purposeful, controlled painting number 3 belongs to another Asian elephant named Methai. Before becoming a painter, Methai was a circus performer in Thailand. She’s a musician as well as an artist and can play several instruments, including the harmonica. Methai is the most prolific elephant artist at the zoo, and like Shanti, she too is all business when she paints: she is known to squint her eyes in concentration.
Painting number 4 was done by Harry, a White-faced Saki monkey. He’s a tree-dweller from the South American rainforest who mastered the art of painting quickly. He works fast, often completing his masterpieces in mere minutes, and tends to be pretty laid-back, although rumor has it he sometimes gets a bit frenetic about his work and ends up with paint all over him once he leaves the studio.
Credit for the last painting on exhibit at TMC goes to Cali the sea lion. The smart, playful sea lions are a crowd favorite at the Houston Zoo, and when Cali isn’t putting on a show or hunting for fishy treats, she’s churning out paintings like the one on display at TMC. She holds a paintbrush in her mouth to create her masterpieces, then hops back into the pool to frolic with her buddies.
Nietzsche said “The essence of all beautiful art, all great art, is gratitude.” After seeing this beautiful art, this great art, I’m grateful for Shanti, Wednesday, Mathai, Harry, and Cali.
Coming soon to a hospital or surgery center near you: drive-by doctoring.
It’s the latest trend in chicanery, in which some health-care workers (namely high-dollar specialists) insert themselves into a case in order to jack up their revenue.

googleimages.com
It’s come to light thanks to this article in The New York Times. Here’s the long-story-short: “In an increasingly common practice that some medical experts call drive-by doctoring, assistants, consultants and other hospital employees are charging patients or their insurers hefty fees. They may be called in when the need for them is questionable. And patients usually do not realize they have been involved or are charging until the bill arrives.”
Here’s how it typically works: you have a medical problem, say breast cancer, that needs to be fixed. You see a specialist and/or a surgeon and do your research. You might even check with your health-insurance provider to ensure that your doctor and procedure are covered. Your doctor’s office also ascertains pre-approval and pre-certification for your surgery. You do your due diligence and assume all your ducks are in a row. Meanwhile. you are consumed with getting your life in order before your surgery date; in my case, in the 2 weeks between being diagnosed with stage II invasive breast cancer at the age of 40 and undergoing a bilateral mastectomy, I stocked the house with groceries and washed every item of clothing in the house; I arranged for rides to & from school and extracurricular activities for my two elementary-school-aged children; I submitted myself to a battery of tests and scans in a series of appointments that constituted a part-time job; I met with my kids’ teachers and guidance counselor to inform them of what was going on at home; I answered phone calls and emails from concerned friends and family and endeavored to keep my people informed of my situation; and I lay awake at night, despite my exhaustion, wondering what the hell my very uncertain future held in store for me.
I did not, however, think to ask if the army of health-care providers and the plethora of services my cancer required were all in-network. I was rather busy wrapping my head around my diagnosis and ensuring that I did everything I needed to do, for myself and for my family. The last thing on my mind was whether I’d get screwed by out-of-network providers charging 20 to 40 times the going rate.
Surprise! Here’s a huge bill for services you neither requested nor consented to, and not paying will ensure sleepless nights, stressful budgeting sessions, and harassment by collection agencies.
Luckily, I had great health insurance at the time I “waged war” on my cancer. Luckily, I happen to live in the epicenter of research and healthcare institutions; my city has some of the best medical schools and the best cancer-care facilities, which correlates to an abundance of first-class docs and hospitals. Luckily, I did not fall prey to drive-by doctoring during my cancer “journey,” but am nonetheless considering this a cautionary tale.
In the NYT article, a man named Peter Drier found himself recovering from back surgery and facing a $117,000 bill from an “assistant surgeon” he never met. Drier did his homework and researched his health-insurance coverage before his surgery, but still found himself a victim of drive-by doctoring.
Patients have their hands full before their surgeries, and some providers are looking to shore up revenue that is increasingly reduced by economics. It’s the perfect storm. Furthermore, hospitals that join an insurance network are not required to provide in-network doctors or services. New York has enacted legislation to protect consumers from drive-by doctoring; let’s hope other states follow. Until then, it’s buyer beware.
Misguided by emotion. Foolishly thinking one more surgery would do it. Clamoring for “the end.”
Although my intellectual side knew it could not be, my psychological side was hopeful that my recent hysterectomy would free me from adjuvant therapy for stupid, dumb breast cancer. My 3 1/2 years of Tamoxifen were bad. Really bad, and got progressively worse. I wrote about my Tamoxifen experience a time or two, including the always entertaining T-Rage. I was a happy girl after kicking Tamoxifen to the curb, but I did worry about the estrogen that was no longer being blocked by the drug, nasty as that drug was.
Removing my girl parts, which is a good thing in preventing breast cancer recurrence, would seem to be the answer, no? Yanking my ovaries meant my body could no longer produce estrogen, which could no longer feed any errant cancer cells that hung around after lopping off both breasts at the ripe old age of 40.
However, as those of us in Cancerland know, being pro-active and doing all you can isn’t enough. It’s never enough.
I’ve surrendered both breasts, both fallopian tubes, both ovaries, my uterus and my cervix in hopes of leaving Cancerland. Cumulatively, I’ve spent more than a month in a hospital bed, and suffered through 267 days of post-hospital antibiotic therapy for that nasty nosocomial infection I picked up along the way. And yet, it’s not enough.
It’s never enough.
While my nonexistent ovaries can no longer make estrogen, now I have to worry about estrogen from my adrenal glands. These two glands are located just above the kidneys in a space called the retroperitoneum and produce small amounts of estrogen. Even though I am now sans girl parts, I still have to think about the fact that my body is full of cells, both healthy ones and potentially cancerous ones, that contain estrogen receptors. These receptors can go haywire when they come in contact with estrogen, and can set off a shit storm called cancer recurrence. My defense against the potential shit storm is yet another drug.
Introducing Femara. It’s an aromatase inhibitor whose job is to find the enzyme that’s required to make estrogen and get rid of it. It’s similar to Tamoxifen in that it protects me from estrogen and has similar side effects: hot flashes, hair loss, joint/bone/muscle pain, tiredness, unusual sweating, nausea, diarrhea, dizziness, and trouble sleeping. It’s different from Tamoxifen in that it’s for postmenopausal gals and it doesn’t increase the risks of blood clots or uterine cancer. It does, however, erode bone density. With these drugs, it’s a give & take. Mostly take.
My cutie-pie oncologist wants me to start taking Femara. Because the 3 1/2 years of Tamoxifen hell weren’t enough. Because surrendering both breasts, ovaries, fallopian tubes, uterus, and cervix weren’t enough. It never ends.
The studies on Femara and recurrence show promise. The two main studies show that Femara reduces the risk of recurrence, increases the span of time before the cancer recurs, and reduces the risk of the cancer spreading to other parts of the body.
All good, right? Wouldn’t you want to do everything you could to reduce the risk of recurrence? Even if it meant taking yet another drug and enduring more side effects for years and years and years?
It’s never enough.
It’s never over.
Yesterday I bid farewell to my uterus, cervix, ovaries and Fallopian tubes. They are gone, baby gone. Well, actually they’re in lab somewhere in the Medical Center, undergoing testing. Hopefully no evil this way comes.
The surgery was easier than I expected (although anything will be, compared to what I’ve endured in the past). As usual, the care was exceptional at The Methodist Hospital. Its slogan is “Leading Medicine,” and those folks practice what they preach.
I was on the labor & delivery floor, which was nice and quiet and had the added bonus of allowing me to peep at the newborns in the nursery as my IV pole and I walked laps around the floor.
One tiny complication (you didn’t really think I’d get through surgery without one, did you?!). Last night my blood pressure dropped and stayed low — 80s over 50s — all night. I must admit, I felt kinda puny. Watching those numbers hover so low as they checked me every two hours was a bit worrisome, but after two bags of IV fluid and a few more laps around the floor, it was back to normal this morning. I was back home barely 24 hours after checking in for surgery.
I’m feeling a bit smug, I must say, after the nurse told me another patient had the exact same surgery as I and she’s nowhere near ready to go home. She didn’t even want to get out of bed, while I was slipping on my flip-flops and packing up my bag to get outta there. To each his own.
Here’s my take on the latest Disney film, but first a disclaimer: I hate Disney films.
Now, before you boo me and flame me and hate me, let me clarify. I hate that Disney films have traditionally relied on the death of the main character’s mother to build the character arc that defines the movie.
Dealing with the death of someone significant (in my case, my sweet mama) sucks. It really sucks. Going to the movies or employing other forms of escapism should distance one from that suckiness, not magnify it, and I’ve been smacked in the face by Disney’s tired mechanism again and again. However, my favorite girl wanted to see Maleficent and she wanted me to go with her, so I girded my heart against Disney’s mean mechanism and took my girl to the movies.
Sufficiently girded, I was crazy-curious about those cheekbones the makeup artists gave the titular character.

googleimages.com
Yowza. That bone structure is sharp. And somewhat distracting.
And those lips.

glamour.com
That lipstick.

maccosmetics.com
Those wings.

gooleimages.com
I am enough intrigued by Maleficent’s messages to look past Disney’s transgressions upon my heart. Most intriguing in this case is the idea that the bad guy (or in this case, the bad girl) isn’t always bad. Or perhaps has good reason to be bad. The line between good and evil is blurred. And while that may be troubling, it’s realistic.
It’s not just realistic, it’s also updated and reflective of modern life, not “once upon a time.” The fairy tale transcends a bedtime story to be indicative of real life. Aren’t we in essence creatures who endeavor to be “good” and do the “right thing” even though forces beyond us sometimes conspire against us? Or is it just me? My instinct when someone cuts in front of me in line is to tap them on the back and tell them to get the hell behind me, to take their turn. Instead, I smile sweetly and gently point out that I believe I was there first. Why, just yesterday while waiting for new tires I saw not one but two different people look at the sign on the door to the work area — the one in big, red letters that says DO NOT ENTER WORK AREA. FOR COSTCO TIRE CENTER EMPLOYEES ONLY — and open the door. They stopped to read the sign, then tried to enter the work area anyway. My first thought was to ask them if (a) they truly do not understand the sign; or (b) if they truly think the sign and its message do not apply to them; or (c) if they truly are so important and pressed for time that they cannot wait for the tire-center employee to leave the perilous work area and come to the safety of the lobby area to serve them. However, I chose none of those options; I minded my own business and let the tire-center employee deal with it. I want to be polite and nonviolent, yet the idiots around me present a challenge. I want to be “good” but have lots of reasons to be bad. I want to be nice, but life gets in the way.
Maleficent knows what I mean. She feels my pain. She’s a sweet, orphaned fairy (gorgeously portrayed as a young fairy by Isobel Molloy) who has yet to grow into those cheekbones (but early on masters the art of choosing the right shade of red for her lips) and who smiles a hugely charming smile as she frolics with her woodland-creature friends.

googleimages.com
Our sweet orphaned fairy goes about her business in the Moors and meets a boy who becomes her friend but later betrays her. He drugs her and takes something precious from her (and no, you did not imagine the hints of rufies and date rape here). His betrayal creates the proverbial woman scorned. As the movie’s narrator points out, the antagonist and the protagonist are one and the same. That blurred line between good and evil reappears.
While Maleficent appears to be a bitter, resentful she-beast hell bent on extracting revenge from the man who wronged her, we could also ask, what about that man? What is his role in her transformation? Is his lust for power and his drive for the throne a cautionary tale about the repercussions of overwhelming greed and hunger for power?
I think so. But I digress.
Whether the woman scorned was born or made into the role of the villain is irrelevant in the face of the idea that maybe, just maybe, we all have a touch of both good and bad in us.
And maybe, just maybe, it’s ok to root for a female bad-guy as we’ve longed rooted for the male versions. They may be bad, but we sympathize with them. We kinda identify with them. Who among us has not been wronged or hurt by someone we love? That’s not to say I want to hang out with Hannibal Lecter or that I condone his predilections, but there are aspects of him that are intriguing, interesting. He’s smart and funny and pretty damn dignified for a man in a scary-looking metal mask. He’s also quite kind to Clarice. I despise him but am intrigued by him. Blurred lines.
Many messages are at work here: that things aren’t always as they seem. People (and fairies) are complicated. Unchecked power and greed lead to ruin. And perhaps more importantly, that the dichotomy between good and evil is not so black and white. Blurred lines.
As anyone who has faced long-term illness or disease will tell you, wading through the medical bills can be a full-time job.
Luckily, I don’t have nearly as many bills to wade through these days. However, in Cancerland, the next expensive test and big bill can be — and usually is — right around the corner. The latest for me was a vaginal ultrasound in March to determine if my ovaries are up to no good after coming off tamoxifen. Yes, that’s right, a vaginal ultrasound. Don’t be jealous. It’s yet another perk for those of us in Cancerland.
I struggled long and hard with tamoxifen. I’ve written about my complicated relationship with the drug many times; most recently about the T-rage I had been experiencing. Like poor Bruce Banner, I was one Hulk smash away from wrecking something for good, and I didn’t like that. I also had serious bone pain that got worse instead of better. I felt as if I were aging at a scary-fast pace. While the bone pain and aging were unpleasant, they weren’t deal-breakers. The T-rage, however, was a deal-breaker.
The T-rage was bad, really bad, but even worse is the increased risk of uterine cancer. For someone with a complicated family history of reproductive cancers, uterine cancer isn’t something I’m willing to risk. I’m not looking for a three-peat here; melanoma in 2006 and breast cancer in 2010 are more than enough for me. Throw in tamoxifen’s potential to cause liver as well and I’m downright spooked (with my affinity for champagne, my liver is likely limping along as it is. No need to tax it any more than my bubbly habit already does.)
I broke up with tamoxifen last fall. After three years, the side-effects were piling up like cars on Houston’s Southwest Freeway during rush hour. As much as I would have loved to have made it to the 5-year mark with Tamoxifen, it was unlikely; even more unlikely was being on the drug for 10 years, as is the current recommendation for pre-menopausal women.
Whether to continue taking the drug was a very difficult decision, and one with which I struggled. In the end, it came down to quality of life. Cancer and its far-reaching tentacles had already taken so much from me; I wasn’t willing to give up the slight hold I had on my sanity. It is a very personal decision. Much like the decisions that go along with surgery options and adjuvant treatments, what’s right for me might not be what’s best for the next person in Cancerland.
I’m far from alone in my decision to stop taking tamoxifen, however. This study of nearly 9,000 women with early-stage breast cancer revealed that only 49 percent made it all the way through five years. Younger women were more likely to quit their treatment, perhaps because of the far-reaching side-effects that come along with the drug.
As nasty as tamoxifen can be, just stopping it doesn’t mean the trouble ends. Because the estrogen my ovaries produce is no longer blocked by tamoxifen, the potential for that estrogen to feed hungry cancer cells is once again a very real possibility. The next-best option is having my ovaries removed, hence, the ultrasound in March that kicked off the latest round of harassment by my insurance company.
Yes, I am grateful to have health insurance and I am very sympathetic toward cancer patients who do not. The one thing that can make cancer more crap-tastic is to have to worry about going broke because of it. Being stressed about money is no fun. Add in all the hype about stress contributing to cancer, and the crap-tastic scenario becomes even crappier.
As was the phone call I received last week from the hospital where I had the vaginal ultrasound to determine what, if anything, was going on in my possibly ill-behaving netherregion. Here’s how it went down:
Her: “Hello, this is YaddaYadda So-and-So with the hospital you had your ultrasound at on March 20, 2014. I’m calling to collect the $508.40 you owe for that ultrasound.”
Me: (silently, to myself: Do not correct her horrible grammar. Let.It. Go. “at on” is not the worst thing a person can say. Even a person trying to collect money.) “Oh, hi YaddaYadda So-and-So.”
Her: “How are you today?”
Me: “Feeling like I’m about to become $508 poorer.”
Her: (silence)
Me: “hello?”
Her: “Yes, I am calling to collect $508.40.”
Me: “I have no idea to what you are referring. I have not received a bill for my portion of the ultrasound.”
Her: “So you did have an ultrasound on March 20, 2014?”
Me: “Apparently so, otherwise I cannot fathom why we would be having this conversation.”
Her: (more silence)
Her: “When can we expect payment for this unpaid service?”
Me: “When can I expect to see a bill for this service?”
Her: “It will be mailed out this weekend.”
Me: “So, you’re calling me to ask me to pay a bill that I have yet to receive?”
Her: “Yes ma’am. What kind of payment can you give me today?”
Me: “How about we wait on that? Maybe until I actually receive a bill?”
Her: “Ok, but when can we expect to receive your payment?”
Me: “Ummm, how about after I receive a bill?”
Her: “When do you think that will be?”
Me: “Am I being punked? Is this conversation for real?”
Her: (silence)
Me: “Here’s how it’s going to work: once I get a bill I will review the bill. Then I will check with my insurance company. Then I will pay whatever I owe. However, nothing is going to happen until I get a bill.”
Her: “Ok. Thank you for choosing our hospital. Is there anything else I can help you with?”
Me: “I’m not sure you’ve helped me with anything yet, so “anything else” is not likely. But thanks for asking”
Her: “Good-bye.”
The very next day, I get another call from another person in the billing department at my hospital. She, too, wanted to know when they can expect the $508.40 I owe. I told her, quite gently, that I have yet to receive a bill and that I had a conversation to the same effect yesterday, with her colleague. She seemed as dismayed as her colleague that I wasn’t ready to fork over $508.40 for a service for which I’d yet to see a bill.
Two days later, still no bill, but yet another phone call from yet another person in the billing department. I told her that she was the third person to call about a bill I had yet to see. I asked her to please put a note in my file that says Do Not Call Me Until the Bill Has Been Mailed. And Then Wait a Couple More Days to Give Me Time to Go to the Mailbox and to Read Over the Bill.
At this point, my patience had worn rather thin.
After doing some investigating with my insurance company, I learned that the claim had yet to be filed. I duly called the billing office of the hospital to report my finding. I left a voice message stating my business; I suppose all the billing representatives were busy on other lines, cold-calling customers asking for payments for bills not yet process, mailed, or received. I felt comfortable ignoring the two voice mails the billing department left me while I waited for the bill to arrive.
Today I got a call from yet another billing representative, telling me that they got my voice mail and were calling me back to take my payment. Here’s how that convo went:
Her: “Yes, I’m wondering how you’d like to pay the $508.40 owed on your account.”
Me: “You mean the $508.40 about which I left a voice mail, saying I checked with my insurance company and no claim for that service on that day by this hospital has been submitted?”
Her: “Yes ma’am. How would you like to pay?”
Me: (silence)
Her: “May I place you on hold, to verify that the claim has been processed?”
Me: “You call me, then want to put me on hold? So you can check to see if there’s a reason for you to have called me?”
Her: “Uh, yes. Ma’am.”
Me: (sigh) “Ok.”
Her: “Ma’am, we show that your insurance company just submitted payment for $1249.10 today. They just paid today.”
Me: “Ok. Great. So we’re done here?”
Her: “Um, I think so, but let me double check. May I place you on hold?”
Me: (sigh) “Ok.”
Her: “Yes ma’am, your insurance company paid the $1249.10. Today. They paid today. Just now. I don’t see that you owe any deductible. But, um. How would you like to pay your portion?”
Me: “My portion of what? You just said I don’t owe any deductible.”
Her: “Um, that’s right. I don’t think you owe anything at all”
Me: “So we’re done here?”
Her: ” Yes. Is there anything else I can help you with today?”
Me: (sigh)
Here’s what I want to know: does the hospital make such phone calls soliciting payment on purpose, hoping the recipient of the call will just pay whatever amount they’re told, right there over the phone? Or is the billing process complicated enough to warrant the kind of confusion that results in a customer receiving multiple phone calls asking for payment for a bill that’s yet to be received?
Or was I being punked?

Yesterday I turned 45. I’m on the far side of middle-aged and am four years into life after cancer. Whatever that means. I suppose I don’t have any idea what life after cancer means, other than the fact that nothing is ever the same afterward. In honor of growing another year older, I decided to read a “young adult” book, to see if I still knew what is young, hip, and/or cool. I had read several glowing reviews of The Fault in Our Stars by John Green. Despite those glowing reviews, I initially resisted reading this book, because I didn’t want to read a book about teenagers with cancer.
But that’s the thing about The Fault in Our Stars. It’s not about kids with cancer. The main characters, Hazel and Gus, have cancer, but the book is about so much more than their respective diseases.
I wondered how Green could write so convincingly and wrenchingly about the role that cancer does play in the book, if he had not been touched by disease himself. So I read an interview with him and learned that he worked as a chaplain in a children’s hospital and met lots of sick kids. In that interview he said, “When I was at the hospital, I met all of these young people who, yes, they were sick, but they were also many other things. They were funny and angry and sad, and they had all of the emotions that any other human has, all the desire, all the wishes. And that was what really resonated with me.”
That resonates with me, too, because it’s true. People who have had or currently do have cancer certainly have the same emotions, desires, and wishes as any other human. However, those emotions are often sent into overdrive, as we must confront things we aren’t prepared for or would rather not face.
Those desires are often perilous because of the uncertainty of our fate. As Gus so eloquently expresses it, “Almost everyone is obsessed with leaving a mark upon the world. Bequeathing a legacy. Outlasting death. We all want to be remembered. That’s what bothers me most, is being another unremembered casualty in the ancient and inglorious war against disease.”
Those wishes play a big part in the book, as the characters are forced to learn a hard truth at a very early age: That life is not fair. Or, as Gus puts it, “The world is not a wish-granting factory.” In the interview I read, Green spoke to the idea of the world not being a wish-granting factory:
“I think cancer in many ways to those of us alive today is similar to what tuberculosis was like in the 19th century. It’s so unfair: It takes the young, it takes the old. Sometimes you live, sometimes you die. And it’s very difficult to make sense of the reasons why it may go one way or another. It’s very, very difficult to imagine it as anything other than just cruel and cold and capricious. And that makes it difficult to imagine the universe as anything other than cold and capricious. And I wanted to be honest about that, because I wanted them to have to face, in the most desperate way, that overwhelming question, as T.S. Eliot called it, of how we’re going to organize our lives and what they’re going to mean.”
Hazel and Gus confront the capriciousness of whichGreen speaks. Gus talks about receiving an 85 percent chance of surviving his cancer: “I know those are great odds, but I kept thinking it was a game of Russian roulette. I was going to have to go through hell for six months or a year and then at the end, it still might not work.” Hazel points out that being her situation was completely different: as a Stage IV cancer patient, her “final chapter was written upon diagnosis. Gus, like most cancer survivors, lived with uncertainty.” I had never before considered that a Stage IV patient might view herself as having a more certain future.
Hazel describes a scene that was very familiar to me during the multiple hospitalizations I had from the post-mastectomy infection: “The first thing they do is ask you to rate your pain on a scale of one to ten. I’ve been asked this question hundreds of times over the years and remember once early on when I couldn’t get my breath and it felt like my chest was on fire, flames licking the inside of my ribs fighting for a way to burn out of my body. A nurse asked me about the pain and I couldn’t even speak so I held up nine fingers. Later, after they’d given me something [for the pain], the nurse said, ‘You know how I know you’re a fighter? You called a ten a nine.’ But that wasn’t quite right. I called it a nine because I was saving my ten.”
Saving my ten.
Another quote that really resonated with me is this:
“Pain is like fabric; the thicker it is, the more it’s worth.”
While that is true, it’s also true that the more it’s worth, the more it costs. That’s why I’m saving my ten. 
David Walmer was a fertility specialist at Duke University who went on a mission trip to Haiti in the early 1990s. While there, he was shocked to learn of the high rate of cervical cancer among Haitian women. A disease that is highly preventable was killing some 250,000 women a year in developing nations, and Haiti led the world in deaths from cervical cancer. Walmer knew he had to get involved.
Walmer returned to work in North Carolina and learned everything he could about cervical cancer, mainly that it can be detected for a decade before becoming untreatable. Detection is easy because unlike many cancers, it grows in a visible spot: on the outside of the cervix. Routine screening via Pap smears is the norm; before Pap smears became the de facto screening tool, cervical cancer killed more women than any other form of cancer. Since the adoption of Pap smears, the death rate from cervical cancer has dropped by 70 percent. The CDC reports that in 2010 in the United States, 11,818 women were diagnosed with cervical cancer. Of those, less than 4,000 cases were fatal. Compare that to the CDC’s breast cancer stats for the same year: 206,966 women and 2,039 men were diagnosed with breast cancer. Of those, 40,996 women and 439 men died from breast cancer. Therein lies the inherent value of a highly visible cancer
If a Pap smear detects abnormal cells, the next step is to examine the cervix via a special magnifying lens called a colposcope. Walmer realized that outfitting underdeveloped nations with colposcopes could make all the difference in preventing cervical cancer deaths, but that getting colposcopes into the hands of doctors in those nations would be unrealistic because of cost, size, and dependence on electricity. Undeterred, he opted to get creative.
He realized that a common surgical tool — the loupe — could provide magnification without electricity. To provide the contrast needed to detect suspicious cellular activity on the cervix, Walmer bought a Halogen bike headlamp and a green filter for a camera and began to tinker.
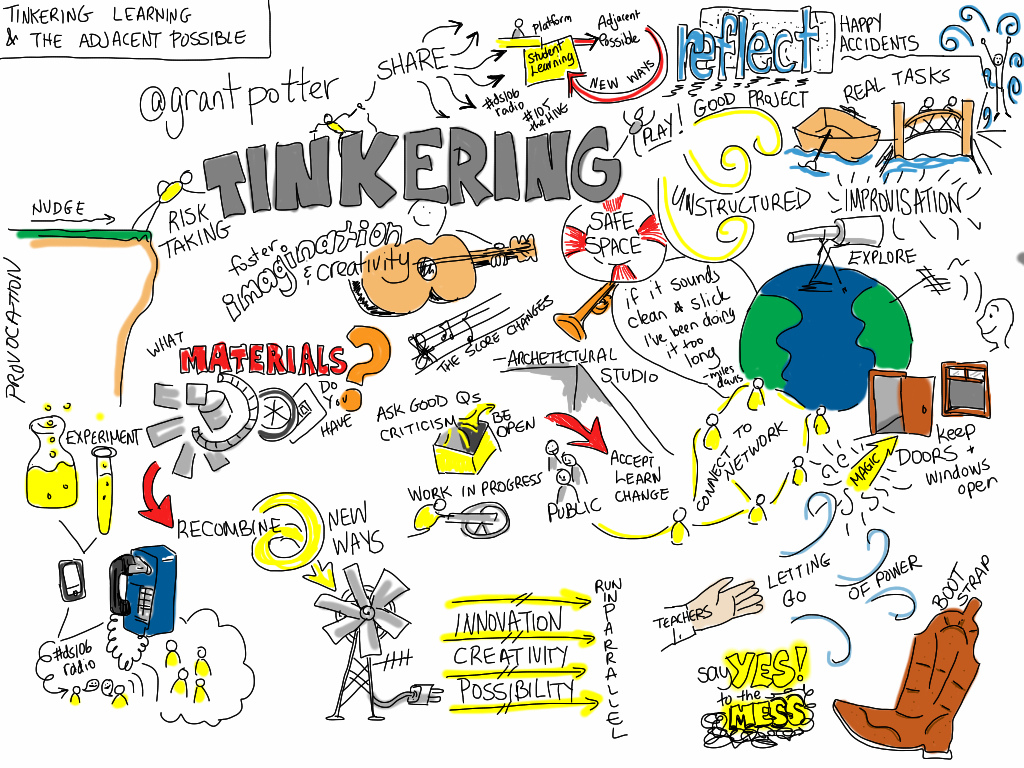
Giulia Forsythe
A colleague at Duke who taught biomedical engineering got wind of Walmer’s pet project and lent some muscle: namely students in his Engineering World Health club. One of those students, Theo Tam, recruited four other students to work on Walmer’s portable colposcope. These four young men were some of the brightest minds in the sciences and engineering student world, yet they were freaked out by the prospect of working on something so closely tied to the most intimate part of female anatomy. Tam says the other guys were willing to take on a multitude of projects designed to improve medical conditions in third-world countries, but not the portable colposcope. “Anything but the V-word,” Tam says. “Imagine the horror.”
Tam also got creative, and convinced the guys to get involved with the parts of Walmer’s project not related to “the V-word”: marketing, finance, and other “safe” parts. Once they got past the horrifying idea of the female body part, the guys got to work. They assembled a prototype colposcope using lenses from a $2 pair of reading glasses, magnification from a $10 pair of binoculars, and lights from a $16 battery-powered LED. The first portable colposcope, named the CerviScope, was born. After a few more tweaks, it was ready to go. With help from a grant from an investment bank, the CerviScope was ready for mass production.
Walmer created a nonprofit, called Family Health Ministries, from his North Carolina home, to get the CerviScope into healthcare facilities in impoverished countries. FHM’s goal is to screen for and prevent cervical cancer. An integral part of achieving that goal is advocating for the HPV vaccine. The American Cancer Society also advocates for the HPV vaccine; read more about it here. The CDC provides compelling evidence for the HPV vaccine: A 2013 study shows that in the 8 years since the vaccine’s introduction, the virus has decreased 56 percent among girls ages 14 to 19. CDC Director Tom Frieden estimates that two-thirds of American girls aged 13 to 17 have not been vaccinated, and that the 2013 study proves that “the HPV vaccine works well, and the report should be a wake-up call to our nation to protect the next generation by increasing HPV vaccination rates.” Frieden warns that the low vaccination rates in the United States will equate to 50,000 new cases of cervical cases; cases that would be prevented with the vaccine.
There are many take-away messages from David Walmer’s story. That easily-visible cancers are much preferred to those that burrow deep into the body’s nooks & crannies. That even the most brilliant scientific male minds are rendered powerless by the female honey pot. That one finds one’s calling in the most unlikely places. And that tinkering definitely pays off. In a very big way.

Illustration by David Benbow

{kind=link}